The 3rd European Congress on Endometriosis, with close to 500 participants from more than 30 countries, was held in Budapest from 17-19 November 2016.
President of European Endometriosis League, Dr Stefan Renner, said:
“It is the time of change. Endometriosis does not change, but our understanding of the disease, the diagnostics and options for treatment do“.
The congress started with a pre-course to renew knowledge about endometriosis with respect to practical and clinical problems, and continued with 2 plenary lectures, 10 lecture sessions, 3 oral communications, 5 national meetings, a four-hour live surgery, and 22 poster presentations.
The three years from the last European Congress on Endometriosis have brought new ideas, new questions, and new knowledge to the field. What follows are some key messages from the congress.
Endometriosis influence on oocyte quality and quantity
Professor Andrea Genazzani, from the University of Pisa, gave a passionate speech with an overview of literature together with his personal points of view.
Professor Andrea Genazzaini, University of Pisa
He believes that it is not just a question of oocyte quantity, referring to studies showing that implantation rates of oocytes from donors with endometriosis are reduced in recipients without endometriosis, while women with endometriosis undergoing IVF treatments involving oocytes from non-affected individuals show normal implantation and pregnancy rates [1,2]. He brings out several steps in oocyte maturation and oocyte environment that have been shown to be altered in cases of endometriosis [3-8].
Professor Genazzani is convinced that our goal should be to start treating endometriosis as soon as the first symptoms occur to avoid reduced fertility. He stressed dysmenorrhea as the most important first symptom.
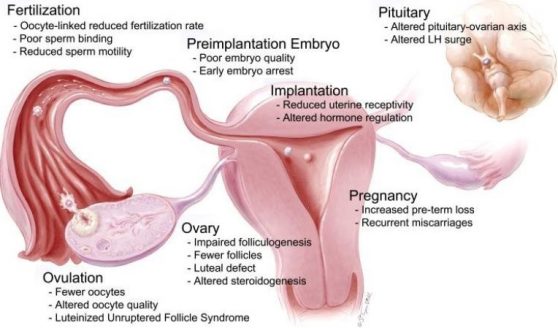
Endometriosis and infertility. Drawing used by Professor Genazzani
From: Stilley JAW, Birt JA, Sharpe-Timms KL. Cell Tissue Res 2012;349: 849

Dr Alfredo Guillen, IVI Madrid
Dr Alfredo Guillen, from IVI Madrid, presented his viewpoint as an IVF-specialist asking if we need a lot of oocytes or just a few good ones.
Referring to professional scientific literature he stresses that endometriosis causes mainly quantitative damage, but in contrast to Professor Genazzani, Dr Guillen is convinced that endometrial receptivity [9,10] and oocyte quality is not significantly affected [11].
Finding the balance between surgery and medically assisted reproduction
There is still no common guideline for diagnostics and treatment of endometriosis. Creating it is a challenge waiting ahead. Hormonal treatments help to relieve symptoms (minimally in cases of deep endometriosis (DE)) as long as they are administered, but real challenges come if women with endometriosis want to become pregnant.
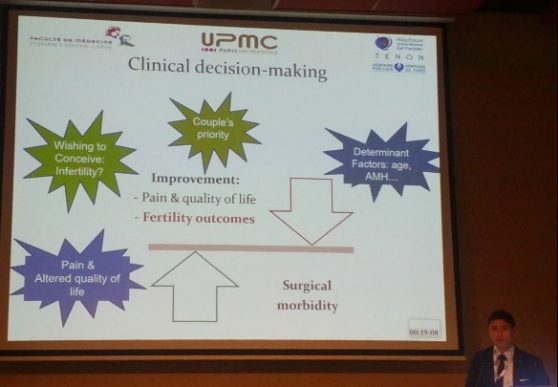
Professor Marcos Ballester, Tenon University Hospital of Paris (France)
Professor Marcos Ballester, from Tenon University Hospital of Paris, talks about the challenges of clinical decision making. He points out that the key challenge is to recognise those women who would benefit most from first-line ART and those who would be helped more by first-intention surgery. This challenge is emphasised by the lack of high level of evidence in the literature. In the future, randomised trials (DE with and without bowel involvement) and predictive models will hopefully help to identify those women better for the right treatment.
According to the information we have now, Professor Marcos Ballester concluded:
- Deep endometriosis without bowel involvement: first-line = surgery
- Women requiring rectal shaving/full thickness disc excision: first-line = surgery
- Colorectal endometriosis: first-line = ART, surgery in case of prior ART failure

Dr Vesna Salamun, University Clinical Center Ljubljana
Dr Vesna Salamun, from University Clinical Center Ljubljana, believes in an integrated therapeutic approach for treating endometriosis-associated infertility. The integrated approach is primary laparoscopic operation combined with secondary IVF, if spontaneous conception fails. This is distinguished from the “surgery prior IVF approach” were surgery is done for a safer and more feasible IVF that is done as soon as possible after operation.
Dr Salamun’s message was that IVF should not be seen as a competing method with the surgical treatment of endometriosis-associated infertility, but as a complementary therapeutic strategy. She advises to wait with IVF after surgery in the case of rather young (up to 35 years) patients who have a normal ovarian reserve and no partner-related cause for infertility. Their study results coincide with previous studies that show the integrated approach gives good results and does not lower the efficiency of IVF if spontaneous pregnancy is not achieved [12-13].
How far can a gynaecologist go?
Due to a growing number of DE operations, new gynaecological teams are involved in the management of bowel endometriosis. A small number of gynaecologists with a solid background in bowel endometriosis are now able to perform various bowel techniques.

Dr Horace Roman, Rouen University Hospital
One of those gynaecologists is Professor Horace Roman from Rouen University Hospital in France. He focuses on the surgical management of endometriosis. He explained that the question is not how far can we go, but more how far we are allowed to go.
Gynaecologists are basically not trained for bowel surgery and general surgeons are not trained for conservative endometriosis surgery. This is why multidisciplinary teams are justified and required by law. He compares those teams of gynaecologists and general surgeons with two singers who sing a new hit.
Delivery after surgery for deep endometriosis
As more and more surgeries for deeply infiltrating endometriosis are developed, the obvious question, how post-operatively decreased elasticity of tissues in the pelvic region can influence the outcome of vaginal delivery, is raised.

Dr Peter Oppelt, Kepler University Hospital
Dr Peter Oppelt introduced the first description on delivery modes after operation for DE [14]. They did not find an elevated risk for perineal or vaginal laceration in women with a history of surgery for deeply infiltrating endometriosis, even when a resection of the rectum or of the posterior vaginal wall had been performed.
Concerning the small number of patients with resection of the rectum because of endometriosis and the possibility of spontaneous delivery, there is still no consensus for a recommendation. Dr Peter Oppelt said,
“My best interpretation of the few data is that after an operation of the rectum the possibility of cesarean section should be discussed with the patient. Definite recommendations cannot be made until we have new and bigger studies.”
Therapeutic alternatives for preserving fertility

Dr Ralf Dittrich, Erlangen University Hospital (Germany)
Dr Ralf Dittrich, from Erlangen University Hospital in Germany, stressed that providing information about fertility preservation is important, especially since technology for fertility preservation is available to almost everyone nowadays.
The main techniques for fertility preservation are cryopreservation of oocytes and ovarian tissue. Dr Dittrich said that it is reasonable to offer these techniques to endometriosis patients as they have an increased risk of infertility, especially when bilateral endometriomas are present.
However, there are some points to be considered. Although freezing ovarian tissue for fertility preservation is an established method for cancer patients, there is no data for endometriosis patients. Moreover, the procedure can be complicated due to possible adhesions, diminished number of follicles in ovaries and it causes additional loss of ovarian reserve. When freezing oocytes, it is essential to freeze oocytes as early as possible because, in all probability, the ovarian reserve will be exhausted earlier than in women without endometriosis.
New therapeutic option: US guided radiofrequency-ablation (RFA)
Dr Sara Brucker, from the University of Tubingen, introduced possibilities of ultrasound guided radio-frequency ablation for treating fibroids. Representing the results of their randomised trial of 50 enrolled subjects, she compared two minimally invasive uterus-sparing treatments- laparoscopic myomectomy and the RFA-procedure.

Dr Sarah Brucker, University of Tubingen
Dr Brucker concluded that prospectively followed patients had statistically significant reduction for both groups and the difference between the two cohorts was not statistically significant after 5 years. There was also no difference in health-related quality of life. On the contrary, RFA is less invasive, presented with reduced pain during recovery, and allowed for a quicker return to work.
Moreover, due to lower invasiveness RFA allows to influence the smallest fibroids, minimising the need for re-interventions. Previously, RFA has also shown good effectiveness in treating symptomatic adenomyosis [15]. In this light, ultrasound guided radiofrequency ablation might be a safe and effective minimally invasive alternative in the treatment of different gynaecological pathologies.
In conclusion
The 3rd European Congress on Endometriosis brought together European leaders in the field of endometriosis. Throughout the congress the impact of endometriosis on fertility was in focus. It was evident that although there has been a great amount of research on endometriosis, many questions remain unanswered.
In order to put together common guidelines in endometriosis management, a better understanding of the disease and best treatment needs to be achieved. We have learned a lot during the last decades, but there is still plenty of work ahead to make treatment of endometriosis more effective and to increase health-related life quality of those patients.
We will see how much has been achieved for the year 2018 when the next European Congress on Endometriosis is held in Turkey.
References
- Navarro J, Garrido N, Remohi J, Pellicer A. How does endometriosis affect infertility? Obstet. Gynecol. Clin North Am 2003;30:181–192.
- Simón C, Gutiérrez A, Vidal A, de los Santos MJ, Tarín JJ, Remohí J, Pellicer. Outcome of patients with endometriosis in assisted reproduction: results from in-vitro fertilization and oocyte donation. A Hum Reprod 1994;9(4):725-9.
- Barcelos ID, Vieira RC, Ferreira EM, Martins WP, Ferriani RA, Navarro PA. Comparative analysis of the spindle and chromosome configurations of in vitro-matured oocytes from patients with endometriosis and from control subjects: a pilot study. Fertil Steril 2009;92:1749–1752.
- Gianaroli ,et al. Predicting aneuploidy in human oocytes: key factors which affect the meiotic process. Hum Reprod 2010;25:2374-2386.
- Borges Jr E, Braga DPAF, Setti AS, Vingris LS, Figueira RCS, Iaconelli Jr A. Endometriosis Affects Oocyte
- Morphology in Intracytoplasmic Sperm Injection Cycles. JBRA Assist Reprod 2015; 19:235-240.
- Cohen J, Ziyyat A, Naoura I et al. Effect of induced peritoneal endometriosis on oocyte and embryo quality in a mouse model. J Assist Reprod Genet 2015;32:263.
- Agarwal et al. The effects of oxidative stress on female reproduction: a review. Reproductive Biology and Endocrinology 2012;10:49
- Garcia-Velasco JA, Fassbender A, Ruiz-Alonso M, Blesa D, D’Hooghe T, Simon C. Is endometrial receptivity transcriptomics affected in women with endometriosis? A pilot study. Reprod Biomed Online 2015;31(5):647-54.
- Díaz I, Navarro J, Blasco L, Simón C, Pellicer A, Remohí J. Impact of stage III-IV endometriosis on recipients of sibling oocytes: matched case-control study. Fertil Steril 2000;74(1):31-4.
- Filippi F, Benaglia L, Paffoni A, Restelli L, Vercellini P, Somigliana E, Fedele L. Ovarian endometriomas and oocyte quality: insights from in vitro fertilization cycles. Fertil Steril 2014;101(4):988-93.e1.
- Barri PN, Coroleu B, Barri-Soldevila PN, Rodríguez I. Endometriosis-associated infertility: surgery and IVF, a comprehensive therapeutic approach. Reprod Biomed Online 2010;21(2):179-85.
- Coccia ME, Rizzello F, Cammilli F, Bracco GL, Scarselli G. Endometriosis and infertility Surgery and ART: An integrated approach for successful management. Eur J Obstet Gynecol Reprod Biol 2008;138(1):54-9.
- Allerstorfer C, Oppelt P, Enzelsberger SH, Shamiyeh A, Schimetta W, Shebl OJ, Mayer RB. Delivery after Operation for Deeply Infiltrating Endometriosis. Biomed Res Int 2016; 2016: 8271452.
- Hai N, Hou Q, Ding X, Dong X, Jin M. Ultrasound-guided transcervical radiofrequency ablation for symptomatic uterine adenomyosis. Br J Radiol 2016;28:20160119.
About the author

Kristi Anderson
Tartu University, Estonia
Kristi Anderson studies in the 6th year at the Medical Faculty of Tartu University in Estonia and is preparing for continuing her studies in the field of Obstetrics and Gynaecology. Attending the 3rd European Congress on Endometriosis was an important signpost in her life.
Her expedition in the world of research has been short, but enthralling. Since the year 2015, she has been part of an endometriosis research team, Competence Center on Health Technologies, and the focus of their research has been complement gene expression alterations in endometriosis. Kristi Anderson was able to show the team’s findings at poster presentation at EEL2016.