The 72nd ASRM Scientific Congress & Expo took place in Salt Lake City on 15-19 October 2016.
The topic of endometriosis was covered in 3 pre-congress courses, 8 roundtables, 3 symposia, and 42 abstracts.
Highlights of the congress included the debate on the necessity of a surgical diagnosis of endometriosis, the surge of miRNAs, the advent of a new treatment, and the presentation of a laparoscopic endometriosis mouse model.
What best serves a patient in pain? Debating the diagnosis of endometriosis.
Visual and histological confirmation of lesions during laparoscopy is currently the gold standard to diagnose endometriosis. However, having a presumptive diagnosis of endometriosis based on history, physical examination, and imaging allows for more rapid triage of patients and start of appropriate second-line therapy while avoiding the risk of surgical intervention.

On opposite sides during the debate, but side by side afterwards.
From left to right: debate chair Dr David Adamson, Dr Eric Surrey, and Dr Michael Diamond.
So which method is preferable? As with most things in life, the best approach lies somewhere in the middle. After the debate, both Dr Michael Diamond (Augusta University, Georgia) and Dr Eric Surrey (Colorado Center for Reproductive Medicine) agreed that each patient’s situation should be considered individually before deciding whether or not to proceed to surgery. Negative physical examination and imaging and absence of (immediate) child wish may dismiss the need for laparoscopy. Evidence of advanced disease, failure to respond to second-line therapy, and management of fertility are indications for proceeding directly to laparoscopy. Dr Adamson (president of the World Endometriosis Research Foundation) added:
“If the only tool you have is a hammer, you tend to see every problem as a nail. If you go to a doctor who is not comfortable with surgery, he will probably use a drug. If you go to somebody who is doing surgery, he will tend to do surgery. So you need to go to somebody who is comfortable with both treatments”.
Short but strong: MicroRNAs as a tool to diagnose endometriosis
In the future, endometriosis might be diagnosed with a blood test, rather than a clinical or surgical assessment. Dr Hugh Taylor (Yale School of Medicine, Connecticut) summarised the state of the art of blood biomarkers for endometriosis. CA-125 is the most commonly cited biomarker. However, at a cut-off of 30 U/ml both the sensitivity and specificity are low. Currently, the investigation of microRNA (miRNA) is a hot topic in the endometriosis field. Several research groups, including the team of Dr Taylor, have recently published manuscripts on miRNAs as biomarkers for endometriosis.

Dr Arne Vanhie, KU Leuven
This year’s Prize Paper Award from the Endometriosis Special Interest Group was awarded to Dr Arne Vanhie (KU Leuven, Belgium).
Using Next Generation Sequencing in 120 plasma samples (endometriosis n = 82, controls n = 38), two panels of six miRNAs were identified discriminating between controls and stage I-II or stage III-IV endometriosis with good sensitivity (79-86%) and specificity (88-92%).
When validated, these models could allow a minimally invasive diagnosis of endometriosis.
The role of miRNAs in endometrial-epithelial dialogue
Other than their role in diagnosis, investigation of miRNAs may provide insights in the link between endometriosis and implantation defects. Dr Mandy Katz-Jaffe PhD, and co-workers from the Colorado Center for Reproductive Medicine investigated the impact of endometriosis on embryo-endometrial miRNA dialogue during the window of implantation using an in vitro co-culture model of blastocysts and epithelial cell monolayers from endometriosis patients or controls. Six miRNAs were down-regulated in the exosomes of co-culture supernatant from endometriosis patients. The target genes that were up-regulated could potentially impact apoptosis and cell cycle arrest.
Deep phenotyping to advance biomarker development for endometriosis
Dr Linda Giudice (University of California San Francisco, and current president of the World Endometriosis Society) summarised the state of the art on biomarkers in urine, menstrual blood, and endometrium, including work of her own group on the aberrant endometrial DNA methylome in women with endometriosis. She also acknowledged our limited understanding of the pathogenesis of endometriosis and its impact on biomarker development.
The blind men and the elephant
The poem “The blind Men and the Elephant” by John Godfrey Saxe (1816-1887) illustrated her point of view. It is a tale of six blind men who all touch different parts of an elephant to determine its nature and find that they completely disagree, “though each was partly in the right, and all were in the wrong”.

In the context of endometriosis we must acknowledge the complexity and different facets of the disease (oestrogen-dependent, progesterone-resistant, inflammatory, immune, pain syndrome, (epi)genetic component, stem cells,…).
Finding different results does not necessarily mean they are conflicting, but may be a result of disease heterogeneity. Dr Giudice emphasised the importance of deep phenotyping to avoid potential confounders such as disease phenotype and location, different ASRM stages, multiple lesion types, as well as the menstrual cycle phase, other concomitant disorders, and the type of symptoms (pain or infertility). For this purpose, the World Endometriosis Research Foundation (WERF) has set up the Endometriosis Phenome and Biobanking Harmonisation Project (EPHect). Collaborative projects with high sample sizes and well-characterised patient groups will be pivotal to put all the pieces of the endometriosis puzzle together.
Exploring Elagolix to treat endometriosis-associated pain
Elagolix is an oral non-peptide gonadotropin-releasing hormone (GnRH) antagonist and was covered in two oral presentations and three posters. Two double-blind randomised placebo-controlled multicentre phase 3 clinical trials were conducted in patients with surgically proven endometriosis and moderate/severe endometriosis-associated pain. Participants were randomly assigned to receive either placebo, Elagolix at a dose of 150 mg or Elagolix at 200 mg. Elagolix inhibited proliferation of the endometrium without causing hyperplasia. The safety profile was described as being consistent with dose-dependent hypoestrogenic effects, with a loss in bone mineral density after six months. The efficacy profile showed a dose-dependent reduction in dysmenorrhea, non-menstrual pelvic pain and endometriosis-associated pelvic pain and – over the course of six months – an overall dose-dependent improvement of the quality of life based on the EHP-30 (endometriosis health profile). These results are encouraging and Elagolix may in the future become a new option in treatment of endometriosis. Oral GnRH antagonists have potential benefits such as obviating the need for injections and allowing better titration of pituitary suppression, however it has to be noted that in these studies Elagolix was only compared to placebo and not to a group of patients receiving GnRH agonists.
Laparoscopy to treat endometriosis-associated infertility

Dr Grace Janik
Reproductive Specialty Center, Wisconsin
The controversies in the surgical management of advanced endometriosis and endometriomas were described by Dr Tommaso Falcone (Cleveland Clinic, Ohio) and Dr Grace M Janik (Reproductive Specialty Center, Wisconsin). Surgical excision of ovarian endometriomas may cause a decline in Anti-Mullerian Hormone (AMH) levels, a surrogate marker for ovarian reserve. Laparoscopic excision of deep lesions and removal of endometriomas have a place in the treatment of endometriosis-associated infertility. To avoid surgical complications, multiple interventions or compromising ovarian reserve, these complex procedures should be done by skilled hands.
Pre-clinical models for endometriosis research
Even though pre-clinical animal models were not prominently represented at this year’s ASRM meeting, the video “Of mice and women: a laparoscopic mouse model for endometriosis” by Daniëlle Peterse et al (KU Leuven, Belgium) received the First Prize for Technical Achievement in Video.
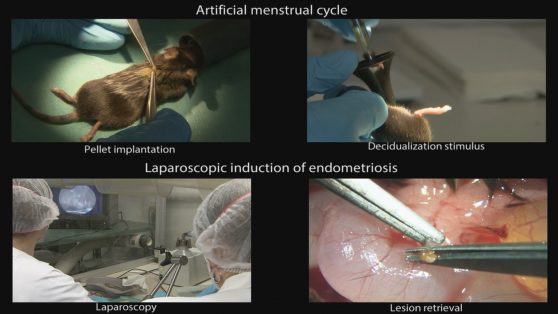
The laparoscopic mouse model for endometriosis, induced with menstrual endometrium. Still frame courtesy of Daniëlle Peterse, KU Leuven, Belgium
The video provided a step-by-step description of endometriosis induction via laparoscopy in mice using syngeneic menstrual endometrium. Laparoscopy allowed minimally invasive and precise placement of the tissue pieces in pre-determined anatomical locations that are typically involved in endometriosis in women. The high intra-abdominal pressure during laparoscopy causing mesothelial damage allowed attachment of the tissue fragments without the need for suturing. This mouse model may be used for fundamental research and drug development.
Conclusion
Despite ongoing investigation and development of potential new therapies, many controversies persist on how to best diagnose and manage endometriosis. Our current understanding of endometriosis is limited and fragmented. Initiatives such as WERF EPHect may prove useful in finding the missing link to elucidate the pathogenesis and diagnosis of endometriosis. MicroRNAs are a hot topic in endometriosis because of their potential as biomarker and their role in the pathophysiology. The continuing efforts to improve the animal models for endometriosis may help solve the puzzle and support the development of novel treatment modalities.
About the author

Dorien O, KU Leuven
Dorien O is a biomedical scientist and PhD student of the Endometriosis Research lab at KU Leuven in Belgium.
It can be a challenge to track her on Google or Pubmed, since her last name consists of only one letter. Her research is focused on the discovery and validation of endometriosis biomarkers using immunoassays and proteomics.
The main objective is to validate biomarker panels in peripheral blood and endometrium in order to develop a minimally invasive diagnostic test for endometriosis.